All published articles of this journal are available on ScienceDirect.

P-Selectin and PSGL-1 in Beta Thalassemia Major Iraqi Patients: A Comparative Study
Authors Info & Affiliations
Abstract
Introduction
Thalassemia, a group of recessively inherited disorders, is characterized by persistent anemia of varying severity and diminished or nonexistent hemoglobin synthesis. Approximately 80 - 90 million individuals, including approximately1.5 percent of the population, are affected by β thalassemia. Beta thalassemia is associated with more than 200 identified mutations. The elevated prevalence of thalassemia in the area extending from sub-Saharan Africa to the Middle East can be attributed to the evolutionary link between malaria resistance and the thalassemia carrier state.
Methods
This study included 100 patients (50 males and 50 females) with β-thalassemia major (β-TM). The subjects were classified into two groups: Group 1 (G1) included individuals diagnosed with a body mass index (BMI) below 30, while Group 2 (G2) included individuals with a BMI above 40. A third group of healthy individuals without any known medical conditions was included as a control group (G3). Blood samples were collected, and an enzyme-linked immunosorbent assay (ELISA) was used to measure the levels of P-selectin and PSGL-1.
Results
The results showed that PSGL-1 may be a more reliable diagnostic biomarker. P-selectin was also found to be useful, although less effective, particularly in identifying obesity-related conditions in individuals with lower BMI.
Discussion
This study aimed to evaluate P-selectin and P-selectin glycoprotein ligand-1 (PSGL-1) as potential biomarkers in Iraqi patients with β-thalassemia major and to assess the effect of obesity on their serum levels.
Conclusion
These findings may help improve the understanding of the relationship between obesity and hematological complications in patients with β-thalassemia.
1. INTRODUCTION
In β-thalassemia, a common form of thalassemia, alterations occur in the β-globin gene, hindering the body's ability to produce β-globin by disrupting transcription and translation, among other mechanisms [1]. Thalassemia is one of the most common monogenic disorders and is particularly prevalent in low- and middle-income countries. Approximately 80–90 million people worldwide, representing about 1.5% of the global population, carry β-thalassemia mutations. Carrier rates vary by region, ranging from less than 1% in most Northern European and North American populations to 5–20% in the Mediterranean, the Middle East, and South Asia [2]. In Baghdad, Iraq, the prevalence of the β-thalassemia trait was reported to be 3.5% in a premarital screening program conducted in 2025. In comparison, regional studies from Pakistan, Iran, and Saudi Arabia have reported trait frequencies ranging from 2% to 5%. These recent data (2024–2025) highlight the ongoing public health burden of β-thalassemia and emphasize the need for effective prevention and screening strategies [3]. Patients with thalassemia generally require lifelong blood transfusions, which can lead to iron overload and may cause damage to various organs, particularly the liver [4]. Over the past few decades, significant progress has been made in understanding the pathogenic mechanisms of hemoglobin switching in β-thalassemia, as well as the physiological processes involved in normal erythropoiesis [5].
P-selectin, also known as PADGEM, GMP-40, or CD62P, is a cell adhesion molecule that plays an important role in mediating cell–cell interactions. It is expressed on activated endothelial cells and platelets. First identified in 1989, it belongs to the selectin family of cell surface glycoproteins, which also includes E-selectin and L-selectin [6]. The expression of P-selectin is tightly regulated, and it can rapidly translocate from the Weibel–Palade bodies of endothelial cells or from the intracellular α-granules of platelets to the cell membrane in response to inflammatory stimuli [7].
P-selectin glycoprotein ligand-1 (PSGL-1) is the primary ligand for P-selectin. It is highly expressed on the surface of leukocytes and exhibits strong binding affinity. This ligand–receptor interaction plays a key role in the “capture and rolling” phase of leukocyte adhesion to the endothelium, which serves as an important stage in the processes of inflammation and immunity. P-selectin also promotes interactions with immune cells by translocating from cytoplasmic granules to the active surface of platelets.
In conditions such as inflammatory arthritis and neuroinflammatory diseases, extracellular vesicles released from activated platelets facilitate the transport of platelet components into body fluids and tissues that are not normally accessible to platelets, such as the central nervous system and lymphatic system [8]. Furthermore, studies have shown that PSGL-1 signaling in neutrophils, which depends on platelet P-selectin, must be localized to the neutrophil uropod to ensure proper positioning of integrins and chemokine receptors involved in intravascular adhesion and crawling [9]. Research using PSGL-1 knockout mice has demonstrated its critical role in P-selectin–mediated neutrophil early adhesion and migration, highlighting its importance in inflammatory responses [10]. Interactions mediated by P-selectin between platelets are also important for maintaining fibrinogen bridges and promoting the formation of larger and more stable platelet aggregates [11]. Studies on erythrocyte interactions with activated platelets have shown that biochemical communication between these cells begins immediately after platelet activation. However, erythrocytes alone cannot initiate platelet activation or enhance recruitment in the absence of a platelet agonist [12]. Overall, the P-selectin/PSGL-1 signaling pathway mediates interactions among endothelial cells, leukocytes, and platelets. These interactions are essential for regulating thrombo-inflammatory and immunothrombotic processes and are controlled by multiple factors, including tissue factors, cytokines, chemokines, and other mediators that influence the functions of endothelial cells, platelets, and leukocytes. [13].
2. MATERIALS AND METHODS
2.1. Study Subjects and Inclusion Criteria
One hundred patients with β-thalassemia major were included in this case–control study and were divided into two groups. Group 1 (G1) included individuals with a body mass index (BMI) of less than 30, while Group 2 (G2) included patients with a BMI greater than 40. The mean ages of Groups 1 and 2 were 38.73 and 35.46 years, respectively. A third group (G3) consisted of 35 healthy individuals without any known disease and served as the control group, with a mean age of 35.33 years. Serum iron and transferrin levels were measured manually. Serum levels of P-selectin and PSGL-1 were measured using ELISA kits (human SELPLG and Elabscience ELISA kits, respectively). Patients’ height and weight were measured in the hospital examination area using a calibrated scale. BMI was calculated according to the following formula: weight (kg)/height squared (m2) [14, 15].
2.2. Exclusion Criteria
All individuals diagnosed with β-thalassemia major who were hospitalized at the Thalassemia Center at Al Karama Hospital in Baghdad were excluded based on other factors that affected their BMI, such as underlying kidney illness, severe malnourishment, a history of food intolerance, and early skeletal issues. The patients were not allowed to participate in the trial
2.3. Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 28 (IBM Corp., Armonk, N.Y., USA). Data were presented as mean ± standard deviation (SD). The normality of continuous variables was assessed using the Shapiro–Wilk test, and homogeneity of variances was evaluated using Levene’s test. The three study groups were compared using one-way analysis of variance (ANOVA). When the aggregate ANOVA produced a statistically significant F-value (p-value < 0.05), Duncan’s Multiple Range Test (DMRT) was utilised as the post-hoc procedure to ascertain which specific group means exhibited significant differences from one another.
Duncan's test was chosen due to its appropriateness for biological and biomedical datasets, providing enhanced power for identifying significant differences across groups with moderately varied sample dispersions. So, in all the tables and figures, distinct superscript letters show that DMRT (p-value < 0.05) shows statistically significant differences between groups. Results were considered statistically significant when the two-sided p-value was below 0.05.
3. RESULTS AND DISCUSSION
Table 1 demonstrates no significant difference in BMI between Groups 1 and 3. A notable difference in BMI was observed between G1 and G3. A significant difference in iron and transferrin levels was identified compared to the control group, as shown in Table 1. A notable disparity in iron and transferrin levels was observed in β-thalassemia group 1 in comparison with the control group was shown in Table 2.
| - |
Group 1 Mean ± SD |
Group 2 Mean ± SD |
Group 3 Mean ± SD |
p-value |
|---|---|---|---|---|
| Number | 50 | 50 | 50 | - |
| BMI (Kg/m2) | 25.86±2.74 | 42.00±1.13* | 28.00±4.37 | ≤0.05 |
| WBCs (103/mm3) | 11.38 ± 0.73 | 10.38 ± 0.63 | 0.38 ± 0.63 8 | ≤0.05 |
| RBC 106 / cmm | 5.38 + 0.53 * | 5.98±0.22* | 0.2 ± 0.4 4 | ≤0.05 |
| PLTs103 /mm3 | 261.6±12.3 | 273±15.4 | 213±13.3 | ≤0.05 |
| Hb (g/dL) | 8.4 ± 1.2 | 9.4 ± 1.0 | 13.2 ± 1.4 | ≤0.05 |
Notes: *Groups with different superscript letters were found to differ significantly according to Duncan’s multiple range test at p-value < 0.05.
Abbreviations: BMI = Body Mass Index (Kg/m2); WBCs = White Blood Cells (103/mm3); RBC = Red Blood Cells (106/mm3); PLTs = Platelets (103/mm3); Hb = Hemoglobin (g/dL); LSD = Least Significant Difference.
| - |
Group 1 Mean ± SD |
Group 2 Mean ± SD |
Group 3 Mean ± SD |
p-value |
|---|---|---|---|---|
| Iron mg/dl |
252.53±95.71* | 252.53±95.71* | 78.86±22.88 | ≤0.05 |
| Transferrin mg/dl |
442.53±47.91* | 434.2 ± 50.72* | 272.4±17.88 | ≤0.05 |
| P-selectin (pg/ml) | 1431.5 ± 293 b | 1621.2 ± 532.8 a | 803.5 ± 193.1 c | ≤0.05 |
| PSGL/1 (ng/ml) | 3703.6 ± 917.6 b | 6090.1 ± 979.5 a | 2917.8 ± 519.6 c | ≤0.05 |
Note: *Groups with various superscript characters differ significantly according to Duncan’s Multiple Range Test at p-value < 0.05.
Abbreviations: PSGL-1 = P-selectin glycoprotein ligand-1; LSD = Least Significant Difference.
Table 1 presents a comparative analysis of the three study groups' levels of Iron, Transferrin, P-selectin (pg/ml), and PSGL-1 (ng/ml). All groups showed statistically significant differences in both measures (p-value < 0.05). Notably, P-selectin levels were markedly elevated in G2 (1621.2 ± 532.8 pg/ml) and G1 (1431.5 ± 293 pg/ml) compared to the control group (803.5 ± 193.1 pg/ml), with the highest concentrations found in patients with morbid obesity (G2), as shown in Table 3. Similarly, PSGL-1 levels followed a comparable trend, with significantly increased levels in G2 (6090.1 ± 979.5 ng/ml) and G1 (3703.6 ± 917.6 ng/ml) compared to controls (2917.8 ± 519.6 ng/ml). In addition, a significant increase was observed in G2 compared to that in G1.
|
Parameters Groups |
P-selectin (pg/ml) | PSGL-1 (ng/ml) |
|---|---|---|
| G1 | 1431.5 ± 293 b | 3703.6 ± 917.6 b |
| G2 | 1621.2 ± 532.8 a | 6090.1 ± 979.5 a |
| Control | 803.5 ± 193.1 c | 2917.8 ± 519.6 c |
| LSD | 189.7 | 785.8 |
| p-value | 0.0036* | 0.0027* |
Notes: *There exists a substantial difference between groups at the significance level of 0.05, shown by distinct letters in the same column.
Groups that have various superscript letters. Duncan's Multiple Range Test indicates that they differ significantly from one another at p-value < 0.05.
G1: Patients with a BMI less than 30 kg/m2.
G2: Patients with a BMI of more than 40 kg/m2.
LSD = Least Significant Difference.
Various methods exist for assessing nutritional status, including weight-for-height, age-for-weight, and height-for-age. Nonetheless, based on standardized BMI results, (BMI) is the most popular method for determining whether adults are healthy, overweight, underweight, or obese. In children with thalassemia, regular blood transfusions can help alleviate complications arising from anemia and support proper growth, development, and overall survival [16]. Repeated blood transfusions are associated with a range of adverse effects. Iron overload is one of them. However, the ability of the human body to efficiently remove iron ions from tissues is limited. As a result, patients receiving frequent transfusions develop continually increasing iron overload. This condition, known as hemochromatosis, can have serious and deadly effects if it is not treated promptly because of the toxic build-up of iron ions in cell structures in vital organs such as liver, pituitary gland, thyroid gland, and pancreas. Additionally, frequent blood transfusions increased the risk of transfusion-transmitted viral infections, such as hepatitis, further complicating the clinical management of affected patients [17]. Repeated red blood cell (RBC) transfusions and the consequent iron overload may result in several endocrine problems, including hypogonadotropic hypogonadism, pituitary gland anomalies, growth hormone deficits, and hypothyroidism.
Iron overload poses significant risks because excess iron accumulation in tissues and organs can lead to dysfunction and, ultimately, organ failure. These complications may contribute to growth impairment in patients, manifesting as being small in stature and having an individual with a BMI < 30 [18]. The increase in platelet count may belong to the substance-p)SP) role in the activation of platelets and the formation of thrombi; SP could lead to platelet activation and aggregation. In addition, platelets exhibit SP immune reactivity that is released upon activation [19]. Furthermore, deficiency or inhibition of the Nuclear receptor -1 (NR-1) of this neuropeptide leads to reduced thrombus formation in vitro, the neurokinin-1 receptor–blocking antibody prevents platelet responses to collagen, suggesting that neurokinin receptor one agonists are produced upon platelet activation and function as such paracrine agonists [20].
The detrimental effects of deferrioxamine are thought to result from its propensity to induce excessive tissue deposition and disrupt iron-dependent enzymes that play a critical role in collagen modification [21]. These disruptions are considered the primary contributors to growth abnormalities [22]. Ineffective erythropoiesis lies at the core of thalassemia pathology, significantly compromising the body's capacity to produce an adequate supply of mature (RBCs), leading to persistent anemia. Residual RBCs, characterized by the accumulation of globin chain precipitate on membranes, exhibit increased susceptibility to hemolysis, thereby exacerbating the severity of anemia [23]. Physicians should thoroughly examine complete blood count (CBC) results, paying particular attention to Mean Corpuscular Volume (MCV) and Mean Corpuscular Hemoglobin (MCH) values, along with considering the patient's family history, to identify potential cases of thalassemia and hemoglobinopathies in individuals with anemia [24].
The level of iron showed high significance in the two patient groups when compared with the control. Overload of iron is the primary cause of mortality in individuals with beta-thalassemia major, necessitating a well-coordinated medical team approach for regular follow-up. These follow-ups are essential for detecting early indicators of iron overload and executing strategies to alleviate them. Iron overload is a severe side effect of thalassemia caused by internal and external factors that interfere with normal iron homeostasis. The leading causes of this illness include increased absorption of iron in the gastrointestinal system, ineffective erythropoiesis, and the frequent requirement for blood transfusions [25, 26]. Regular blood transfusions dramatically increase the body's iron levels and are necessary for treating anemia in patients with thalassemia. Each transfusion contributes roughly 200-250 mg of iron, creating an accumulation of surplus that the body cannot eliminate, ultimately causing systemic iron overload [27, 28]. Elevated ferritin levels were directly associated with the buildup of reactive iron ions within the tissues of these patients. The “second disease” is the term used to describe the oxidative damage to erythrocyte membranes caused by this iron overload, which sets off another pathogenic process.
The present study showed a notable elevation in P-selectin levels in individuals diagnosed with β-thalassemia major [29]. These results agree with (Ansharullah et al., Haji et al., and Graham et al.,) described that there were increased fractions of platelets that display the P-selectin activation marker in flow cytometric studies in β-thalassemia patients [29-31]. The results of this study showed a significant increase in P-selectin levels in splenectomies of β-thalassemia major patients when compared with non-splenectomized patients, and the reason for this may be reflected in the state of endothelium activation and destruction, which enhances platelet activation [30-32]. Ataga et al., [33] revealed that patients with splenectomy thalassemia have a shorter platelet lifespan than healthy individuals. Individuals undergoing splenectomies for trauma may have a reduced platelet lifespan due to increased platelet consumption, usually related to active thrombotic disease and hypercoagulable states [34]. P-selectin plays a pivotal role in inflammation by facilitating leukocyte adhesion to the endothelium, activated platelets, leukocyte migration, cytokine release, and secretion of growth factors at the injured site. In addition, numerous researchers have elucidated the role of p-selectin in arterial thrombogenesis by forming substantial, stable leukocyte-platelet aggregates. Taher et al. [35] have indicated that splenectomies and repeated blood transfusions are important risk factors for thromboembolic events, and this is increased in thalassemia intermedia patients, platelet activation resulting from the reduction of endothelium-derived nitric oxide (NO), which causes decreased blood flow and vasoconstriction.
This study demonstrated that neutrophil activation enters an intermediate sticky state when P-selectin ligates PSGL-1. As a homodimer, PSGL-1 is formed via a covalent disulfide bond between the extracellular cysteine residues of its two subunits. PSGL-1 dimerization is essential because P-selectin and PSGL-1-expressing cells cannot interact if a cysteine residue mutation disrupts this mechanism. Additionally, under flow conditions, this disruption prevents cells that express PSGL-1 from rolling on immobilized P-selectin [36]. The relationship between P-selectin and its specific ligand, (PSGL-1), is a vital element of the innate immune system. Among other associated conditions, it can set off maladaptive processes that are essential for the biology of sickle cell disease(SCD), metabolic syndrome, stroke, cardiovascular disease, and venous thromboembolism [37]. Recent progress in the management of (SCD) encompasses the application of humanized monoclonal antibodies designed to proficiently obstruct the binding of P-selectin and P-selectin glycoprotein ligand-1 (PSGL-1), thereby promoting their interaction. This approach lessened the painful vaso-occlusive crises (VOC) that patients were having. In this context, our objective was to investigate whether serum P-selectin (sP-selectin) levels could serve as a biomarker to identify SCD patients who would derive the greatest benefit from this innovative medicine [38].
Table 4 and Figure 1 present the receiver Operating Characteristic (ROC) curve analysis for assessing the diagnostic performance of the P-selectin and PSGL-1 biomarkers. The area under the curve (AUC) values indicated strong diagnostic accuracy for both biomarkers. The PSGL-1 result demonstrated an outstanding AUC of 0.959 (p-value = 0.0013), and P-selectin showed a robust AUC of 0.804 (p-value = 0.0026). The optimal cut-off value for P-selectin (951 pg/ml) achieved a sensitivity of 78.3% and specificity of 82.1%, whereas PSGL-1, with a cut-off of 3162 ng/ml, exhibited remarkably high sensitivity (97.5%) and specificity (93.4%). These results indicate that PSGL-1 could serve as a highly reliable biomarker for identifying individuals with a lower BMI in clinical settings.
| Groups | AUC | SE | p-value | Cut-off | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| P-selectin (pg/ml) | 0.804 | 0.044 | 0.0026* | 951 | 78.3% | 82.1% |
| PSGL/1 (ng/ml) | 0.959 | 0.018 | 0.0013* | 3162 | 97.5% | 93.4% |
Note: *Groups that have various superscript letters are very different from each other according to Duncan’s Multiple Range Test at p-value < 0.05.
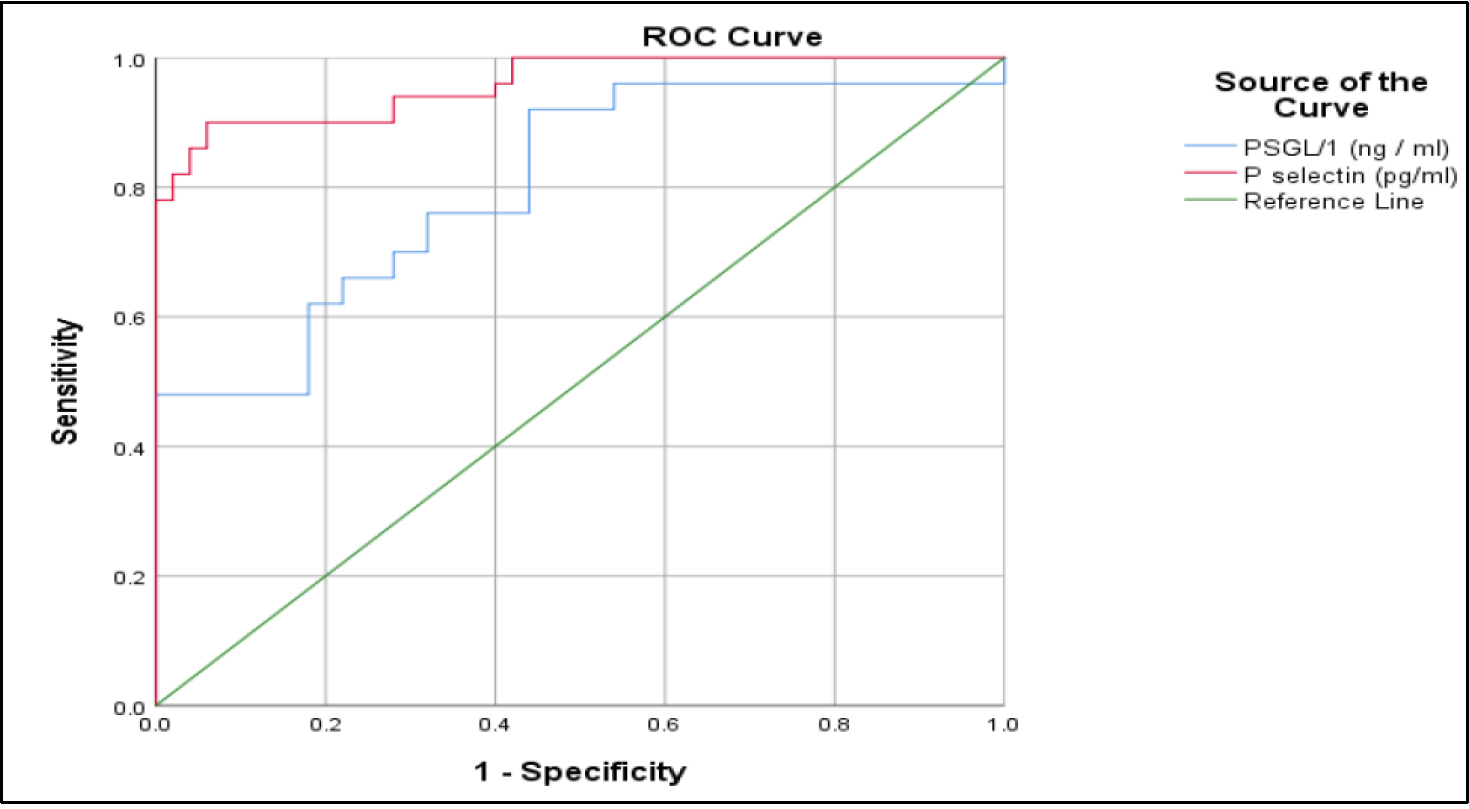
ROC Curve of P-selectin (pg/ml) and PSGL-1 (ng/ml) for G1.
The PSGL-1 ROC curve revealed that it was a great way to find out what was wrong. It goes all the way to the upper left corner of the picture, which shows a perfect test with 100% sensitivity and specificity (AUC = 1.0). This study demonstrates that PSGL-1 is an excellent biomarker for identifying people with a low BMI. The P-selectin curve is also very good in diagnosing because it has a big difference above the reference line (green line), which implies it does a good job of showing the difference between the G1 and control groups.
Table 5 and Figure 2 present the ROC curve analysis for the diagnostic accuracy of P-selectin and PSGL-1 biomarkers in G2 (patients with a BMI > 40 kg/m2). The data suggest that both biomarkers are quite good at diagnosis, with P-selectin having a robust AUC of 0.909 (p-value = 0.0046), sensitivity of 88.7%, and specificity of 93.6% at a cut-off value of 968 pg/ml. PSGL-1 had complete diagnostic accuracy, with an AUC of 1.0 and 100% sensitivity and specificity at a cut-off value of 3860 ng/ml. These results show that PSGL-1 is the best biomarker for accurately determining the difference between the G2 and control groups. It has great predictive ability and does not yield false positives or false negatives. The excellent performance of both biomarkers, especially PSGL-1, emphasizes their prospective applicability in clinical diagnostics for BMI-related diseases, particularly in cases of morbid obesity.
| Groups | AUC | SE | p-value | Cut-off | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| P selectin (pg/ml) | 0.909 | 0.033 | 0.0046* | 968 | 88.7% | 93.6% |
| PSGL/1 (ng/ml) | 1 | 0 | 0 | 3860 | 100% | 100% |
Note: *Groups with different superscript letters indicate statistically significant differences according to Duncan’s Multiple Range Test at p-value < 0.05.
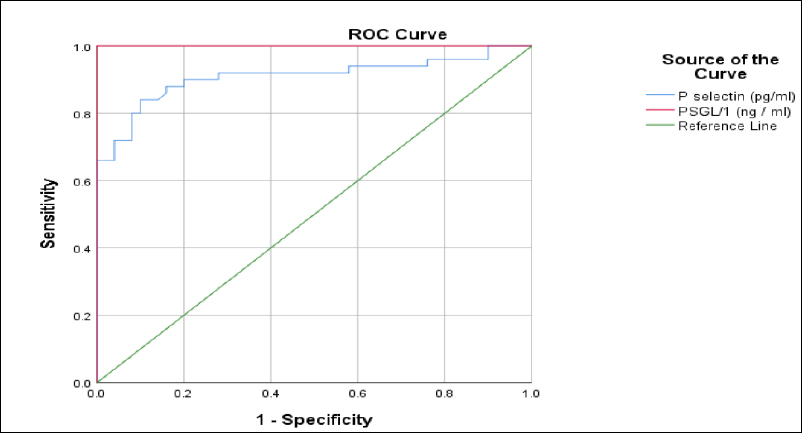
ROC Curve of P-selectin (pg/ml) and PSGL-1 (ng/ml) Biomarkers for G2.
Table 5 and Figure 3 display the correlation analysis with P-selectin (pg/ml) and PSGL-1 (ng/ml) (G1, G2, and G3). Pearson's correlation coefficient exhibited a significant positive correlation within the G1 group. (r = 0.689, p-value = 0.0129), indicating a robust correlation between P-selectin and PSGL-1 in individuals with a BMI of less than 30 kg/m2. On the other hand, there was no significant connection in the G2 (r = 0.189, p-value = 0.1934) and control groups (r = 0.2539, p-value = 0.0634), as shown in Table 6. This means that the association between the two biomarkers was not statistically significant in these groups. These results suggest that the interaction between endothelial activation and leukocyte adhesion may be more significant in individuals with a lower BMI, possibly indicating a separate pathophysiological process compared to those with a higher BMI or in healthy controls.

Correlation Analysis PSGL-1 with p-selectin G1 (BMI < 30 kg/m2), G2, G2 and G3.
|
Group P-selectin (pg/ml) vs. PSGL-1 |
G1 | G2 | Control |
|---|---|---|---|
| r: Pearson correlation | 0.689 | 0.189 | 0.2539 |
| p-value | 0.0129* | 0.1934 NS | 0.0634 NS |
Note: *Groups with different superscript letters differ significantly according to Duncan’s Multiple Range Test at p-value < 0.05.
G1: Patients with a BMI less than 30 kg/m2.
G2: Patients with a BMI of more than 40 kg/m2.
In G1, a notable positive connection was identified (Pearson correlation = 0.689, p-value = 0.0129), indicating a robust relationship between P-selectin and PSGL-1 levels in patients with a reduced BMI. The trend line shows that P-selectin levels go higher when PSGL-1 levels go up. This suggests that there may be a link between endothelial activation and leukocyte adhesion in this group.
In G2, the correlation between PSGL-1 and p-selectin was weak and nonsignificant (Pearson correlation = 0.189, p-value = 0.1934). The data points were widely scattered, and the flat trendline reflected the absence of a clear relationship between the biomarkers in individuals with BMI > 40 kg/m2. This finding may indicate that in morbidly obese patients, the regulatory mechanisms governing these biomarkers differ, or other factors may modulate their expression.
In G3, no significant correlation was observed (Pearson correlation = 0.2539, p-value = 0.0634). Although the trend line shows a slightly positive slope, the p-value indicates that this relationship may be attributed to random variation, as illustrated in Fig. (3).
4. LIMITATIONS OF THE STUDY
Despite the valuable findings of the present study regarding the relationship between P-selectin and PSGL-1 in patients with β-thalassemia major, several limitations should be considered when interpreting the results. The study was conducted on a relatively limited number of participants recruited from a single thalassemia center in Baghdad, which may limit the generalizability of the findings. In addition, some clinical factors that might influence biomarker levels, such as disease duration, transfusion history, and iron chelation therapy, were not evaluated in detail. Therefore, further studies with larger sample sizes and multicenter participation are recommended to confirm and expand these findings.
CONCLUSION
In the present study, P-selectin and PSGL-1 levels were proposed to be significant in patients with beta-thalassemia. P-selectin and PSGL-1 levels have been found to be positively correlated in people with beta-thalassemia major across the two study groups compared to healthy control subjects. P-selectin and PSGL-1 levels were significantly lower in patients with a lower BMI. This strong correlation supports the hypothesis that elevated PSGL-1 levels contribute to or reflect increased endothelial activation as indicated by P-selectin, highlighting a potential mechanistic link between leukocyte adhesion and vascular inflammation. Based on the results and the ROC analysis for P-selectin and PSGL-1 across the three groups, the findings suggest that these markers may point to a possible interaction between them.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: R.A.: Writing - Reviewing and Editing; J.A.: Data Collection; S.A.: Data Analysis or Interpretation. All the authors reviewed and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| PSGL-1 | = P-selectin Glycoprotein Ligand-1 |
| BMI | = Body Mass Index |
| SD | = Standard Deviation |
| RBCs | = Red Blood Cells |
| SCD | = Sickle Cell Disease |
| VOC | = Vaso-Occlusive Crises |
| ROC | = Receiver Operating Characteristic |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Research Ethics Committee, College of Education for Pure Sciences (Ibn Al-Haitham), University of Baghdad, Iraq [No. 3964 in 12/6/2025].
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants prior to their inclusion in the study.
AVAILABILITY OF DATA AND MATERIAL
The data supporting the findings of this study are available from the corresponding author [R.A] upon reasonable request.
ACKNOWLEDGEMENTS
The authors would like to thank all the participants who took part in the study.

